Opus Nuclei's Garden
Powered by 🌱Roam GardenManagement of incidental unruptured intracranial aneurysm
Metadata
Title:: Management of incidental unruptured intracranial aneurysms
Author(s):: Shelley Renowden, Richard Nelson
Publication:: British Medical Journal
Date:: June 3rd, 2020
Space:: Neurosurgery Medicine
Background::
What was the context for this research?
The widespread use of MR has led to the increasingly frequent diagnosis of intracranial aneurysms. Although most are small (<7mm) /and will never rupture/, yet their recognition causes anxiety, and their optimal management remain controversial.
Most of the incidental unruptured intracranial aneurysms (UIAs) develop most frequently at the branch of the basal cerebral arteries, in patients usually between the fourth and sixth decades of life.
What has been studied or determined already?
This review does not apply to symptomatic unruptured aneurysms.
This review does not apply to fusiform, dissecting, mycotic, traumatic and paediatric aneurysms.
Only one UIA will rupture each year for every 300-500 persons with an aneurysm. Thus, a critically important part of the clinical decision-making is to identify the subgroup of patients at most risk of UIA rupture.
The most robust information currently available Population, Hypertension, Age, Sex, Earlier subarachnoid haemorrhage, and Site (PHASES).

Another study has confirmed that 85% of aneurysms with diameter below 7 mm remained stable and did not grow during 10 years of follow-up.
A diameter of 5-7 mm is generally considered the threshold for treatment but the decision also rests on other factors such as age, aneurysm location and morphology, family history and comorbidities.
The risk of a growing aneurysm rupturing is 5 to 55 times that of a stable aneurysm.
After initial detection, 10-12% UIAs grow within 3 years, 45% after 19 years.
Methods::
What was the objective?
To identify the subgroup of which the UIAs's risk to rupture is more prevalent. PHASES score (as seen above) does not include several other risks, such as the aneurysmal size, because PHASES only established that this risk rises above a threshold diameter of 7 mm.
A different measure was used: ELAPSS score.
1507 conservatively managed patients with 1909 UIAs, from 10 centres in five countries with a follow-up of 5782 patient years, the Earlier subarachnoid hemorrhage, Location, Age, Population, Size, and Shape (ELAPS) score uses reported risk factors to predict aneurysmal growth at 3 and 5 years.

How did the author(s) collect data?
Looking at the data from PHASES analysis and ELAPSS.
Conclusions::
What did the author(s) learn overall?
Decision-making through multidisciplinary team to determine the risk of aneurysm rupture is imperative.
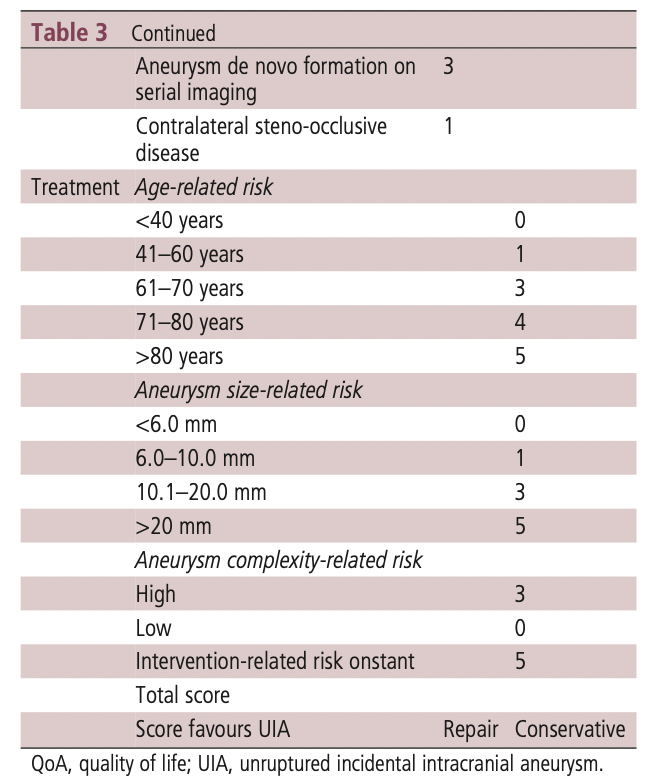
UIATS framework is helpful for the team's assessment. UIATS was derived from a multidisciplinary group of 69 neurovascular specialists using a Delphi consensus to develop a comprehensive scoring model for management recommendations for UIAs.

Screening: screening is recommended for familial aneurysms, autosomal dominant polycystic kidney disease and aortic coarctation, especially among the higher-risk person, such as female, cigarette smokers and hypertensives.
It’s interesting that generally, to screen outweighs the benefit of not screening. The psychological stress, the clinically insignificant treatment (the optimal management is conservative).
Keypoints::
Evergreen Notes If the neurovascular multidisciplinary team does not consider UIA treatment to be beneficial, or if the patient declines it after a detailed discussion of risk and benefit, then conservative management should include treatment of vascular risk factors and non-invasive angiographic follow-up in selected cases.